This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
CMS Policy Changes to Reduce Costs Financial pressures are rising as CMS implements the updated Version 28 Hierarchical Condition Category (HCC) model , which introduces changes aimed at limiting types of codes that are most used for up-coding or over-coding to help rein in spending. Document why you believe that. ” – Dr.
Physicians spend a significant amount of time on administrative work, from writing letters to handling insurance documentation. She estimates that this prompt saves her up to two hours per week , and sometimes even more when demand is high. Follow-up in three months with repeat labs. Jacob Mathew, Jr.,
This comprehensive guide provides hospital and revenue cycle leadership with vital insights on preparing for CERT audits and establishing processes for compliant documentation. This section delves into the specific criteria and expectations set by CERT audits, emphasizing the need for meticulous attention to detail and documentation accuracy.
Dereck Paul is the co-founder of Glass Health, a start-up in San Francisco that offers artificial intelligence chatbot services to doctors looking to ease the burden of routine processes, such as patient documentation. “We need these folks not in burnt-out states, trying to complete documentation,” Paul told NPR.
Staying up-to-date with the latest practices, regulations, and medication management techniques is essential to providing the highest quality of care. Our update class ensures that youre up-to-date with state and federal regulations, helping you stay compliant and avoid potential legal issues.
So, she started documenting her studying process on social media. “I Beggs shared the videos on TikTok where she quickly racked up hundreds of thousands of views. She now has over 600k followers on the app. She said she feels a responsibility to show up for her audience now that she’s built such a devoted following.
I often say to patients (as I apologize for documenting while I get to know them) that I had sworn as a medical student never to be the doctor that types during visits—and when I first became an attending, I held to that. Ideally, I would have a schedule where I could document in the time after a patient leaves the visit.
According to the American Association of Medical Audit Specialists (AAMAS) , a medical billing audit is a process to determine whether data is in a providers health record and by appropriate and referenced medical policies, documents, or support services listed on a providers bill. Also known as chart audit or charge review.)
What can we learn about the left shift of activity from this document? More patient-initiated follow-ups, greater use of the NHS App, and GPs to support patients activating choice of treatment provider are also included. to 4M, with a payment of 20 per advice and guidance request for general practice attached.
The number of healthcare data breaches keeps going up year after year. They should also keep up with the latest healthcare IT news, including the HIPAA Journal , to make sure your system is up to date. These data breaches have affected millions of patients, putting their sensitive healthcare information at risk.
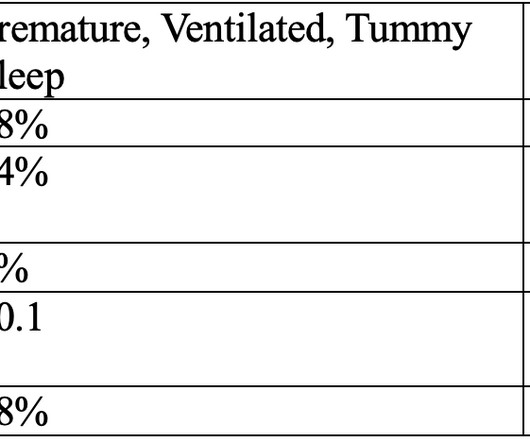
For example, Bergman reports a 2002 study in which ventilated premature babies were placed to sleep on either their tummies or backs, and the following states were measured: quiet sleep, active sleep (which is less restorative than quiet sleep), crying time, number of stress responses (startle, tremor, and twitch), and oxygen saturation.
MaineHealth recently announced it is using AI to automatically record conversations between doctors and their patients during a check-up or follow-up visit. We end up doing what we went into medicine for,” she said. But a new artificial intelligence program could do away with this practice for good.
Here’s a brief explanation: Credentialing with private insurance is often insurer-specific, meaning each company may require different documents or processes. Having these documents ready and in one location can help you stay organized. Organizations like CAQH make it easier to streamline standard documentation.
As healthcare systems become more complex, physicians are spending more time on administrative tasks, including clinical documentation. Team documentation is a powerful way to streamline patient visits and EHR data entry so the entire team can focus on delivering excellent care. What is team documentation?
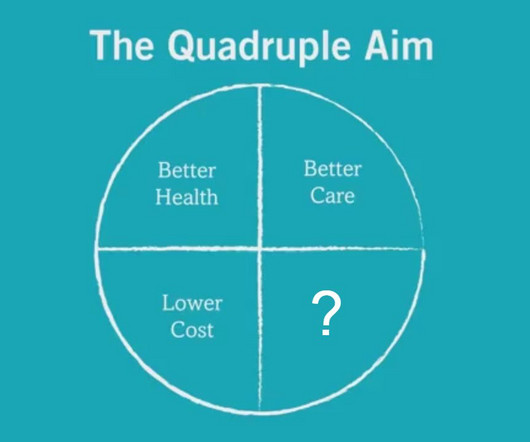
Popular solutions include improving documentation efficiency (a pain point for physicians) and care team coordination. Use pre-visit planning and pre-appointment lab testing to reduce time wasted on the review of follow-up results. The post What is the Quadruple Aim of healthcare?
The Impact of the Two-Midnight Rule on Denials At the 2024 HFMA Annual Conference, we asked healthcare executives if they’re seeing any changes following the CMS Two-Midnight Rule, particularly in denials. Compliant documentation has also become more challenging. Another issue is “inpatient only” procedures.
Those are the words of a Manchester-based Practice Manager who was talking to us following a recent article by Kay Keane asking What is a Practice Manager Worth?. The reality of a Practice Managers day One of the comments responding to Kays article sums up the issues Practice Managers face. last night.
To take action, followup promptly on overdue accounts, review and optimize your billing processes to reduce delays, and consider implementing automated reminders for patients and insurance companies. Compliance and audit reports help you monitor adherence to coding, documentation, and billing standards.
Specifically, we’ll discuss how AI can: Automate Clinical Documentation Support Clinical Decision-Making Triage Patient Communication Diagnose Medical Images Automate Routine Tasks Each topic includes a Software Spotlight, highlighting practical tools that illustrate AI’s impact in real-world settings.
Document medical histories and reason for the visit. Educate patients about managing their health conditions and following physician instructions. Afternoon: Follow-Up: Call patients to remind them of upcoming appointments. Followup on lab results and inform patients of their results as instructed by the physician.
A well-maintained and up-to-date patient database contributes to the overall accuracy and efficiency of the revenue cycle. Accurate coding and documentation process Ensuring staff members are well-trained in accurate coding and documentation is critical to preventing coding errors that could result in claim denials or delays in reimbursement.
When diagnoses are reported only using enrollees’ HRAs and HRA-linked chart reviews and there are no follow-up visits, procedures, or tests, HHS-OIG is concerned that the diagnoses may be inaccurate and therefore the payments made by the CMS may be improper. HHS-OIG’s analysis of MA encounter data identified 1.7
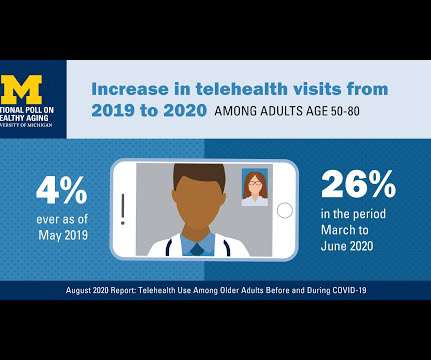
A growing proportion of older patients are engaging in virtual health care visits, and once experienced, patients are generally open to more telehealth in their personal mix of medical services in certain situations — to followup procedures, for repeat primary care and chronic care follow-up, and increasingly, for telemental health.
Wrapping up your practice for the New Year includes: Reconciling all accounts accurately Sorting out outstanding claims Updating patient information These measures will prevent discrepancies that lead to financial loss, reduce mistakes, and speed up the claim approval process, allowing your practice to continue running without glitches.
BioPlus Specialty Pharmacy Services has proposed a settlement to resolve a class action lawsuit that was filed in response to a 2021 data breach that exposed the data of up to 350,000 patients. BioPlus disagreed with the allegations; however, a settlement has been proposed to bring the legal action to an end.
While we often focus our blog articles on streamlining clinical documentation , managing the deluge of messages in your EHR is equally important. For the average PCP seeing 20 patients per day, that adds up to over 13 hours per week. Use Message Templates Dont type the same response over and over.
Coding and clinical documentation have never been more important in healthcare. “We We rely heavily on our coding quality team to onboard new coders and get them up to speed on our quality standards,” said Jake Hess, Senior Director of Revenue Cycle Shared Services at Spectrum Health. Coding is high value — and in high demand.
Coding and clinical documentation have never been more important in healthcare. “We We rely heavily on our coding quality team to onboard new coders and get them up to speed on our quality standards,” said Jake Hess, Senior Director of Revenue Cycle Shared Services at Spectrum Health. Coding is high value — and in high demand.
This being an academic publication, two footnotes informed us that dangling money in front of our eyes can cause people to see what you want to see and come up with an elastic justification for truth. When a new billing code pays more to individual surgeons, significant change swiftly follows, even if only in documentation.
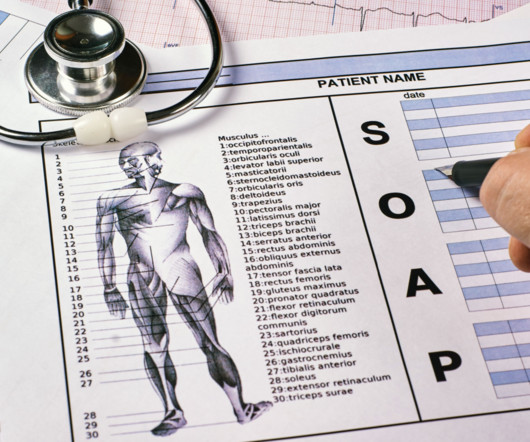
It may be appropriate to say that more data and follow-up sessions are needed. Check out Valant’s clinical documentation features to learn more. Plan : Further diagnostic tests and other tasks are included here, along with proposed treatment including patient education, medications, further therapy, and so on.
Mobile apps for physicians can enable communication with patients and other providers, enhance medical education, inform clinical decision-making, and streamline documentation. What providers are saying: “As a medical student wrapping up my third year, this was my GO-TO reference source for clinical rotations.
Youve found the best EMR for your specialty and streamlined your documentation workflow. Knowing the right medical practice software tools – for scheduling, documentation, clinical decision support, and more – will make your life much easier. Streamline medical practice scheduling with Amion What if you enjoyed scheduling?
” With all of these concerns, it’s vital that providers and billing departments understand and follow the key elements of proper medical billing compliance to run a successful practice. Following health insurance policies and procedures. ” “Do I have all the correct patient information?” The result?
Reviewed by Becky Byrns , CHDS, CHDP-S, CEHRS, MSK and Healthcare Documentation, Health and Wellness Program Manager at CareerStep. Precise and accurate documentation is critical in healthcare and medical transcriptionists play a vital role. The transcription key provided by the client showed the lab test and value “IB 4.4.”
It follows a structured curriculum that covers the following aspects of Microsoft Office: Word : Ideal word processing application, allowing you to prepare and edit documents easily. MOS training in Word equips you with advanced formatting skills, enabling you to create polished documents with tables, graphics and styles.
But another patient side-effect of COVID-19 has been the digital transformation of many patients , documented by data gathered by Rock Health and Stanford Center for Digital Health and analyzed in their latest report explaining how the public health crisis accelerated digital health “beyond its years,” noted in the title of the report.
A 2023 IGNUX report states that hospital coding mistakes make up 63% of medical billing errors. Leveraging electronic health record (EHR) systems incorporating up-to-date coding resources can significantly minimize coding errors and improve billing efficiency.
While the document sets out a vision for integrated, community-focused care, it provides little in the way of clear guidance for GP practices, leaving them uncertain about how they fit into the evolving system. The publication of the Neighbourhood Health Guidelines for 2025/26 has once again left general practice in the dark.
Failing to follow best practices for therapy notes and progress notes can have legal and professional repercussions. The following is not an exhaustive list and state laws may apply, so check regulations in your state. What’s the difference between them, and is your practice compliant with the privacy regulations for each type?
This approach can free up internal resources, reduce time to market, and provide access to niche skills, especially in emerging technologies such as artificial intelligence, blockchain, and the Internet of Things. Scalability Outsourced teams can flex up or down based on project phases.
Reducing duplication errors in medical claims documentation. Automation enables the electronic submission of claims and supporting documents, allowing insurers to review and process claims more quickly. Automated systems ensure compliance by following industry standards and HIPAA regulations throughout the claims process.
Sometimes the answer is obvious: For a company that services hospital machinery, key equipment that is not up and running can translate into delays in diagnosing and treating patients. Which customers should receive immediate follow-up? Who should “own” the follow-up process? Be intentional.
The bad news is that if claims are not handled, the average cost to rework a claim is $25.20, which quickly adds up. Claim denials can occur for various reasons, including incorrect patient information, coding errors, lack of prior authorization, incomplete documentation, and non-covered services. At Health Prime, we can help!
Class members can claim up to $10,000 as reimbursement for documented expenses incurred as a result of the data breach. The stolen data related to customers who made purchases between June 6, 2017, and July 30, 2017, and included names, addresses, dates of birth, drivers license numbers, and other ID documents.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.












































Let's personalize your content