This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
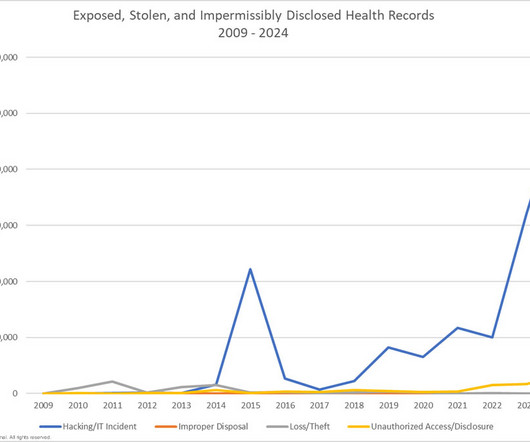
Lake Washington Vascular was unable to determine exactly what information was viewed or extracted from its systems and said the information likely compromised included names, dates of birth, addresses, diagnostic test results, medical histories, diagnosis and treatment information, payer identification numbers, and government-issued identifiers.
Typically, home healthcare has covered (definitionally and in terms of reimbursement) services addressing activities of daily living, durable medical equipment, and hospice. Enter the second chart, which expands what we traditionally have called “home healthcare” into new areas for care at home.
While there are many available NP career choices, the family nurse practitioner (FNP) is a trendy option among nurses seeking to become primary care providers with the authority to diagnose illnesses, order diagnostic tests, prescribe medications, and manage the care of patients across the lifespan.
These settings include nursing homes, rehabilitation centers, assisted living facilities, hospices, and even in-home health care. CNAs most often work in hospitals, but they also can work in other settings where patients receive long-term care or need assistance with daily living activities.
1,500,000 Settlement 2012 Blue Cross Blue Shield of Tennessee $1,500,000 Settlement 2012 Phoenix Cardiac Surgery $100,000 Settlement 2012 The Hospice of Northern Idaho $50,000 Settlement 2011 Cignet Health of Prince George’s County $4,300,000 Civil Monetary Penalty 2011 General Hospital Corp. & million 2020 California Anthem Inc.
As an EBM and diagnostic reasoning obsessive, I often see this as a 2X2 table with the patients knowledge in the columns and the doctors as the rows: Most commonly, both doctor and patient know when the end of life is near — square A. Occasionally, these visits are more difficult and frustrating than sad.
Medical training introduced me to a whole menu of smells -- both diagnostic tools and reminders of times in my career. [i] It was in room 23 that she first raised the possibility of hospice. i] This is one of my favorite slides about the diagnostic smells. [ii] Doctors in training learn to use their senses to make diagnoses.
I think one thing that’s overlooked a lot of time is hospice because that’s like a totally different thing. ” Or you could have a short term thing, but then you gain tremendous value from it. It’s also hard. Emotionally, it’s very difficult. [24:49] 24:49] Definitely, it takes you out of your comfort zone.
Medical training introduced me to a whole menu of smells -- both diagnostic tools and reminders of times in my career. [i] It was in room 23 that she first raised the possibility of hospice. i] This is one of my favorite slides about the diagnostic smells. [ii] Doctors in training learn to use their senses to make diagnoses.
As an EBM and diagnostic reasoning obsessive, I often see this as a 2X2 table with the patients knowledge in the columns and the doctors as the rows: Most commonly, both doctor and patient know when the end of life is near — square A. Occasionally, these visits are more difficult and frustrating than sad.
Knowing what I know now, and having the diagnostic tools that now exist, could I have saved her? He had declined hospice care until the end and would not even accept “do not resuscitate” status. I consulted a cardiologist, a neurologist, a nephrologist, and a rheumatologist. Could I have convinced her to get treated?
⬇️ Learn More About Charlotte Grinberg, MD Dr. Charlotte Grinberg is board-certified in Internal Medicine and Hospice and Palliative care. She currently works as hospice medical director in Maryland. She has also enjoyed advising biotech diagnostic companies in stealth mode between clinical shifts.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.

















Let's personalize your content