This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Say what you’re looking for and what the risk of discharge is in every single progress note. Build Multidisciplinary Teams for Discharge Planning Hospitals can streamline patient care by creating multidisciplinary teams focused on discharge efficiency. Every day, in every note, say why this patient can’t go home yet.
The C-MORE/PHOSP-COVID collaborative group published their results in an important journal—called The Lancet Respiratory Medicine They screened nearly 3000 patients and found about 250 patients who had been admitted and then discharged for COVID-19. The paper is open access so you can see it yourself.
Wilcoxs journey into digital health started with a simple observation: patients in the post-anesthesia care unit were experiencing unnecessary delays in discharge, leading to longer hospital stays. Our goal is to help healthcare professionals get to the right decision faster while also reducing variability in care, Loomis explained.
as more patients get discharged to hospital-for-home and more acute-care workflows that fall on burdened caregivers (that is, family members and friends). Here is ECRI’s list of patient safety concerns a decade ago in 2015. Many more of these have to do with “technology” and devices (e.g., With 3 in 5 U.S.
Cost reduction strategies in BPCI focus on linking payment to performance, utilizing predictive analytics and interprofessional collaboration to lower expenses while maintaining high-quality care. At its heart, the BPCI program emphasizes strong collaboration between healthcare providers as essential for enhancing patient experiences.
Within just 11 months of going live, Baptist Health received the Epic Gold Star Level 10 award, a testament to their operational excellence and collaborative culture. Success Relies on Collaboration At the foundation of Baptist Health’s successful Epic implementation was their culture of collaboration.
We’re still facing the same types of denials, especially with short stays where payers push back post-discharge.” Be on the lookout for post discharge audits as the Medicare Advantage plans do not have to follow the two-midnight presumption.
Prepared Health’s platform enables hospitals to connect, collaborate and react in real-time with the multiple providers involved in a patient’s care post discharge including post-acute, […].
In this role, burn nurses can better assess the needs of their patients post-discharge, anticipating potential problems like lack of transportation, living conditions without heat or electricity, or unstable food resources.
The C-MORE/PHOSP-COVID collaborative group published their results in an important journal—called The Lancet Respiratory Medicine They screened nearly 3000 patients and found about 250 patients who had been admitted and then discharged for COVID-19. The paper is open access so you can see it yourself.
A compliance measure calculates the percentage of patients discharged in the appropriate inpatient or observation bed status—a determinant that can result in major financial repercussions if misclassified. The goal for the compliance measure is to have over 95% of discharges compliant.
George tells us about being discharged home after dealing with heart failure in the hospital. The Lumify transducer plugs into the midwife’s tablet and captures a clinically fine image to collaborate in real-time with a doctor at another location. Take George and Audrey. This has utility for both patient and provider.
Deeply committed to providing evidence-based, high-quality, compassionate, cost-effective patient care through constructive multidisciplinary collaboration and quality improvement. Extensive history as a travel nurse lends itself to readily and seamlessly adapting to novel environments, EMRs, teams, and clinical systems.
Notably, some of the providers involved in the collaborative have said that their hospitals don’t like that they’ve been decreasing emergency department visits and hospitalizations because it hurts the hospital’s finances.
million over five years to examine, with her collaborators, the efficacy of telemedicine services among people recovering from post-intensive care syndrome. Following ICU discharge, patients have problems lasting months to years that often go unaddressed,” Boehm says.
To succeed in health care, interdisciplinary communication and a collaborative mission of nursing practice can result in better partnerships with hospital leadership. per discharge. Obtaining Magnet status can be expensive for smaller institutions. This translates into an added $1,229,770–$1,263,926 in income per year.
In one case, the company has been collaborating with a health system operating 23 hospitals. In the coronavirus pandemic, hospitals want patients to be (appropriately) discharged home from hospital as soon as possible. The willingness is there now,” Roy found, due to the disruption of COVID-19.
For early discharge monitoring , being moved from inpatient monitoring to home monitoring with follow-up care and support, again in the comfort and safety of that patient’s home. Today, Verizon announced its entry into the smart ring marketspace in collaboration with Ultrahuman’s Ring AIR product line.
Immediate Access to Clinical Support Virtual nurses regularly assist with tasks that do not require physical proximity to the patient, such as patient-family education, completing admission and discharge tasks, and participating in two-person verification processes.
Key Takeaways Bundled payment models promote collaborative healthcare and aim to improve care quality while controlling costs, but implementing these models can be challenging due to the need for enhanced coordination among providers.
By your final year, you can admit, treat, and discharge patients on your own and do some procedures without supervision. The goal is never to reach the point of knowing everything but rather to know your limits and when you need additional expertise or collaboration. Refer to AAMC for the training requirements for specialties.
Since healthcare software developers create a new application without collaborating with other application engineering teams, creating custom interfaces meant different languages and communication gaps. But these companies opted for several developers for innovating applications for different applications.
Assessing communication and collaboration. Surveyors will look for structured and unstructured types of care coordination to assess how well the care team members communicate and collaborate to provide better patient care. As part of discharge planning. In broad terms, it’s care management through teamwork.
Discharged to community. Process changes in which the OASIS is reviewed in a more thorough manner or collaboration is occurring between clinicians after the start of care occurs. Measures based on the Outcome and Assessment Information Set (OASIS) contribute to 35% of the TPS and are based on the following OASIS items: Dyspnea.
If you instead said that you “changed the sheets immediately after patients were discharged to ensure swift turnaround time and help meet patient care needs,” that demonstrates how you think ahead, take initiative, and support the work of the team and the hospital, as well as its patients.
Communicating clearly about medication requirements during transitions of care — either from one hospital setting to another or during a hospital discharge — helps prevent errors. But creating and sustaining an organizational culture that values and emphasizes teamwork and collaboration will achieve greater success in the long term.
Physician’s offices offer a friendly and collaborative atmosphere, making them an excellent choice for those who enjoy building relationships with patients and working closely with a small healthcare team. They may perform tasks such as drawing blood, collecting specimens, and assisting with patient admissions and discharges.
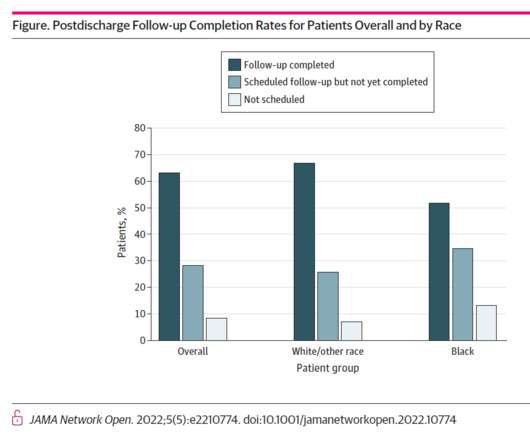
Amidst bullish forecasts for the promise of hospital-to-home discharges, the ability for many patients to make this migration would be a difficult bridge to cross. Patients who reported at least one SDoH concern were less likely to complete a physician follow-up visit post-discharge than patients who reported no SDOH concerns.
Having identified an early condition decline, bedside nurse leaders working in various clinical settings collaboratively work with SWAT RNs to promptly stabilize and prevent patient injury and death. Early detection of patients experiencing physical decline is the hallmark of the SWAT RN role. and HgB- 7.2 and HgB- 7.2
They monitor patients’ conditions, administer medication, and convey self-care and discharge information. Educating patients Patients’ lack of compliance with post-discharge self-care routines — including wound management, medication regimens, and occupational therapy — is a common source of preventable errors in health care.
If these four experience-flows were positive, the patient would be discharged from hospital more likely to recommend the provider to friends, family, and social networks…generating trust. That re-shaping happened through experiences of the hospital’s clinical functions, caring behaviors, operations, and overall culture.
Healthcare providers can order groceries for a patient’s meal plan upon hospital discharge or to manage a chronic condition at home. Among Instacart’s strategics for I-Health is to scale the product Care Carts, which enables health care providers’ and caregivers’ ability to order groceries on behalf of another person.
It involves communicating and collaborating with patients, their families, and their health care teams to ensure that the patient’s needs and preferences are met and that the best possible outcomes are achieved. What is care coordination? Deliver high-quality care that is consistent with the best evidence-based standards of practice.
Collaborating with them means giving them access to healthcare data. It supports inpatient care needs such as real-time tracking of patient information, patient admission and discharge, and management of complex medical data. Net issues mean slow work, downtime, and going down with the system.
Example: SOURCE Collaborative explores non-healthcare factors that may impact blindness from diabetes By using SDOH to enrich clinical research , SOURCE found that lower levels of affluence in a patient’s residential community was associated with progression to blindness.
Students either in MCIM or in my other classes on campus are doing work on discharge planning tools, research for rare disease platforms. We have this required practicum project that several people last year submitted business plans for. I was just on a call about a new technology to use voice to help your mom take her meds.
This was rather eye-opening, as it takes an enormous amount of work and collaboration necessary to pull together a functional disaster preparedness plan. I spent five days in the hospital and was discharged home on oxygen. I met so many amazing people who donated their time and expertise to the project.
Because people go to the hospital, they receive care, get discharged, and then they’re in the community with whatever resources they have. Nursing schools, hospitals, students, and different health organizations follow, listen, or collaborate with nurses at work. So I did a lot of bridging the gap.
Patients are facing health care costs that may result in multi-thousand dollar bills at discharge (or death) that will decimate households’ financial health, particularly among people who don’t have health insurance coverage, covered by skinny or under-benefited plans, and/or lack banked savings for medical spending.
Looking at how maternal care and mental health intersect requires the collaboration of obstetrics and behavioral health care teams. A Personal Story of Maternal Mental Health.
New "Medical Readiness" Button in Transition Planning Tools Connect Care provides a set of integrated supports that can help clinicians anticipate and plan for a patient's discharge from hospital. Designed to facilitate multidisciplinary collaboration, the Transition Planning Package improves communications within and across encounters.
Expanded Access to Improved Transition Planning Tools Connect Care provides a set of integrated supports that can help clinicians anticipate and plan for a patient's discharge from hospital. Designed to facilitate multidisciplinary collaboration, the Transition Planning Package improves communications within and across encounters.
It involves collaboration across diverse healthcare disciplines so as to orchestrate comprehensive management plans focused on all aspects pertinent to juvenile health outcomes. Hospitals and Cancer Centers In hospitals and cancer centers, oncology nurses work collaboratively with interdisciplinary teams to deliver comprehensive patient care.
During discharge planning when documenting in the electronic medical record, the care team should perform a thorough assessment of behavioral and social risks and act on any identified risks to ensure appropriate evaluation and care. This would involve putting resources into place prior to discharging the patient — not just checking a box.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.











































Let's personalize your content